
characteristics of stab wounds

Epigastric stab wound
Source: Dr Michael Surgrue, Trauma Service, Liverpool Hospital
Stab wounds are incised wounds where the length of injury on the surface is less than the depth of penetration into the body, and are the result of a thrusting action, where the force is delivered along the long axis of a narrow, pointed object. The force of impact is concentrated at the tip of the implement, and the sharper the tip, the easier it will penetrate the skin.
The weapons of choice in the majority of assaults – both domestic and ‘on-the-street’ include lock knives, sheaf knives and kitchen knives.
Characteristics of stab wounds
- Clean cut edges
- One or both ends pointed
- Non-pointed end may be squared off or split (fish tail or boat shaped defect)
- Often gape (related to skin elasticity and Langer’s lines)
- Cross section of weapon may be illustrated when edges of wounds opposed
- Underlying bone may be scored by blade
- Abrasions may be present
- Frequently shows notching or a change in direction (caused by relative movement of the knife and body)
assessing stab wounds - wound dimensions

Knives - Andy Warhol
Source: www.quillp.com
When examining a stab wound, the length of the wound should be measured to the nearest mm. The wound should be measured and documented again following apposition of its edges, as this may provide additional information about the wound profile, particularly in skin which has not suffered from excessive 'drying artefact'. Steristrips, or similar clear tape can be used to gently appose wound edges in preparation for photography.
It should be noted, however, that any attempt to determine the dimensions of a knife from the wound are fraught with inaccuracies, due to the effect of elasticity of skin shrinking slightly on withdrawal of the knife (by up to 2mm). In addition, where the blade has entered the skin at an oblique angle, the length of the entry slit may be longer than expected.
Solid organs, such as the liver may retain the characteristics of a knife causing a wound, and at autopsy, for example, these wounds can add to the information obtained from an examination of the surface characteristics of the stab wound.
Stab and other incised wounds should be documented in terms of their anatomical position, and their relative position(s) to fixed anatomical landmarks, such as the top of the sternum, or the ‘point of the shoulder’. Further descriptive methods include the location of a stab wound in relation to the crown or heel, and the midline.
The use of pre-printed body diagrams and or drawings are excellent supplements to the medical notes, and access to digital photography in most accident and emergency units makes the photographic documentation of wounds with quality images is becoming a realistic proposition for even the busiest of casualty physicians.
Stab wounds are said by some authors to ‘gape open’ depending upon their anatomical location. Lines of tension in the skin are determined by the relative orientation of elastic and collagen fibres, and the cleavage lines of Langer correspond to body surface creases.
Cox (1941) reviewed, and 'mapped' (by making 22,600 puncture wounds in cadavers) the cleavage lines, and noted that it was Dupuytren who first observed (in 1834) that there was a disparity between the shape of an instrument and the shape of the skin wound produced by it. Wounds made with a conical instrument were linear, not circular, in shape and that the direction of these wounds differed in different parts of the body. The lines of cleavage, however, were first published by Langer in 1861.
It was postulated that the lines of cleavage were due to the intrinsic arrangement of collagen fibres in the skin - the majority running parallel to the long axis and the remainder interlacing. The orientation of these fibres was further investigated by Haut (1989), examining the tensile strength (and failure) of rat skin. The tensile failure (giving rise to lacerations) depended upon location, orientation, age and strain rate.
Tensile strength of skin oriented circumferentially (along the lines of cleavage) exceeded that oriented longitudinally (i.e. parallel with the body axis).
Surgeons are well aware of the effect of cutting across Langer’s lines – the wound gapes open, as opposed to cutting in the direction of these elastic fibres under the skin surface – the resulting wound does not gape.
However, Hunt (2003) adds a word of caution – experimental mapping of Langers lines on stab victims revealed a disparity between the orientation of stab wounds and gaping. The gaping wounds did not align ‘correctly’, and so limited information can be gleaned from this phenomenon. Indeed, he also notes that in addition to Langer’s lines, there are 33 other types of lines of tension described in the literature.
Byard et al (2005) describe 3 cases in which wound morphology was substantially altered by their relationship with lines of skin cleavage.
A knife that has not fully entered the skin will only produce a wound of a size corresponding to that part of the blade that has penetrated – this will not necessarily represent the maximum dimensions of the knife, and any interpretation of knife wounds must take this into account. Where there are several wounds, measurements taken from each wound may go some way towards building up a composite picture of the true dimensions of the weapon.
assessing stab wounds - type of weapon involved

Soviet NR40 Military knife
Source: Wikipedia

Double edged bladed knife
Source: Wikipedia
Ormstad et al (1986 pp. 529-542) examined the types of knives used in homicides in Sweden, and found that in 62% of cases, the knife was picked up at the scene.
They were invariably the sorts of knives that are found around the home, such as carving knives etc. In the remaining cases, either the perpetrator or victim had brought the knife with them as either protection or for aggressive use.
These weapons tended to include domestic kitchen knives, as well as lock knives and such implements as screwdrivers etc.
Karlsson (1998 pp.21-32) found that weapon knives were most likely to be used in homicides (as opposed to suicides) in Sweden (such as bayonets, stilleto knives and daggers), and that suicides were most likely to use kitchen knives or razor blades.
Kitchen knives were used in just under 40% of homicides and a razor blade in less than 1% of cases.
|
Object |
Suicide (%) |
Homicide (%) |
|
Kitchen knife |
33 |
39 |
|
Razor blade/ razor |
31 |
0 |
|
Sheath knives/ tool knives |
9 |
29 |
|
Pocket knife |
6 |
0 |
|
Glass splinters |
2 |
2 |
|
Weapon knives |
1 |
7 |
|
Scissors |
1 |
1 |
|
Several objects used |
1 |
4 |
|
Not known |
16 |
18 |
Sharp objects used in sharp force homicide and suicide in the Stockholm area (1983-1993) (Adapted from Karlsson 1998)
Knives with single cutting edges such as kitchen knives cause wounds that have a clearly pointed edge, with the opposite edge being squared off ('boat shaped' defect) or split (often termed a ‘fish tail’).
Hunt (2003) believes this ‘fish tailing’ to be artefactual, and has demonstrated experimentally that these marks can be reproduced by rocking the blade within the wound.

Single edged blade inserted into modelling clay (note square edge, and sharp cutting edge, profiles at different depths of penetration)
Source: Richard Jones (WIFM)
Green (1978 pp.161-163) carried out research into the biomechanics of knife wounding, and found that the ‘ideal’ weapon was a short, thin bladed stiff knife of approximately 7cm long (such as the commonly encountered ‘lock knives’ or small 'sheaf' knives) and that larger knives required significantly more force to penetrate skin – their tip were observed to ‘catch’ on clothing. Cheaper domestic ‘kitchen’ knives tended to bend and break on impact.
Pathologists and forensic physicians are often asked whether a knife was serrated or not. Serration markings can sometimes be made out where a knife has been drawn over the skin surface, for example at the termination of the wound. In practice this finding is not at all a constant feature of wounds made by serrated knives – they are usually indistinguishable from wounds caused by other single-edged knives.

Serrated kitchen knife (note impression of blade penetration into modelling clay and serration marks from 'dragging' knife accross clay surface)
Source: Richard Jones (WIFM)
Ciallella et al (2002) pp.82-87 report the characteristics of wounds caused by a survival knife – with serrations on the non-cutting edge (that act as a ‘saw’).
It can be seen that when the knife enters the skin at a shallow angle, the saw edge comes into contact with the skin giving rise to excoriated ‘slashes’, and a ‘V’ shape can be made where the knife is partially removed and moved within the wound. This relative movement occurs often in knife attacks which are dynamic, and the victim, attacker and knife may move relative to each other at any stage of the attack, giving rise to difficulties in interpretation and reconstruction of the events leading to the wounds under investigation.
Knives or weapons with 2 sharp edges (‘double edged’ blades) such as bayonets and ceremonial daggers are rarely encountered in UK forensic practice, but show pointed edges on both sides of the wound, or a spindle shaped entry slit tapered at both ends.
Knives with blade guards (usually referred to as hilt guards) can also produce distinctive bruising at one edge of the wound, where the guard has impacted against the skin, particularly where the skin is supported, such as on the chest wall.
Such hilt marks, however, are uncommon, and Hunt and Cowley (1991 pp.107-112) only identified them in 3% of cases. Knife guards are also sometimes in surprising places (ie. on the opposite side of the knife that would have been expected).
Bruising may also be present where the assailant’s fist impacts against the skin during the stabbing.
Wounds caused by other implements such as screwdrivers and chisels may have abraded edges, and ‘Phillips type’ screwdrivers may give rise to wounds that are stellate in outline. However, dull square shaped objects may also result in stellate wounds due to splitting of the skin at the wound edges, so any interpretation of these sorts of wounds must be made with caution.
Ice picks produce wounds that are sometimes mistaken for small calibre gunshot wounds – i.e. rounded defects surrounded by a thin circumferential rim of abrasion.
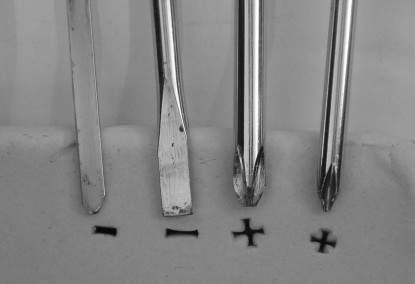
Impressions made by various screwdrivers in modelling clay
Source: Richard Jones (WIFM)
Factors to be assessed regarding the type of weapon involved in sharp force trauma (Knight 1996)
- Length, width and thickness of the blade
- Single/ double edged
- Degree of taper from tip to hilt
- Nature of back edge e.g. serrated or squared off
- Face of hilt guard
- Any grooving, serration or forking of blade (e.g. hooked tip of knife in the 'Wigwam' murder case)
- Sharpness of edge and extreme tip of blade
assessing stab wounds - movement of the knife in the wound
Knives are rarely pushed into the body and withdrawn at exactly the same angle (unless the victim is incapacitated at the time of the assault).
In addition, both the assailant and victim are in a highly charged state during an altercation, and movements of the principle parties are therefore highly fluid. Knife wounds reflect this dynamic situation, and are often ‘V’ shaped or irregular - also referred to as ‘twisting cuts’.
Rocking movements of the knife during an assault distorts the appearances of the wound, and the resultant defect is often much larger than would otherwise have been created by the same knife in a more static situation.
assessing stab wounds - depth of thrust
The clinician is interested in the depth of injury, in order to assess which deeper structures may be at risk.
Compressible body parts, such as the chest wall or abdomen can indent during a knife attack, and structures deep within that area can be damaged at a depth that at first indications seems to be beyond the reach of the suspect weapon.
Estimations of depth of thrust may be further complicated when it is considered that blades with back edges that are sharpened for a few millimetres will cause spindle shaped incisions when the knife is only introduced superficially, but when thrust deeper, it gives rise to a wound with a squared edge typical of a single edged weapon.
Depth of penetration estimations are therefore difficult to make, and may only be confirmed at autopsy, or during surgical dissection.
assessing stab wounds - direction of thrust
Reconstruction of knife attacks attempts to assess the relative positions of the assailant to the victim, and the characteristics of the surface wounds may assist in determining angle of impact. For example, the edges of one side of the wound may be ‘undercut’ or ‘shelved’ when a knife enters the skin at an angle.
If a knife is passing from below the umbilicus towards the nipple, for example, subcutaneous tissue may be visible at the inferior (bevelled) surface, and not the superior (undercut) surface.
Other indications of direction of impact include superficial abrasions or small ‘nicks’ in the skin at the entry point. The examination of clothing may also reveal useful information about the direction of thrust, and should be retained and examined in all cases.
Attempts have been made by researchers over the years to find alternative methods of demonstrating both depth of penetration, and the general characteristics of a knife wound, with a view to matching the measurements with a suspect weapon.
Such techniques have included the use of latex solutions being poured into the wound tract. However, these techniques have proved unsatisfactory due to the leakage of the solution through tissue planes and around the wound.
Methods using probes have also proved difficult, and have sometimes damaged the tract, thus distorting it’s dimensions. Clearly, non-invasive and non-destructive techniques would be ideal, and newer imaging modalities, such as MRI may provide alternative solutions in the future. (For example, see Thali et al 2002).
assessing stab wounds - degree of force
A question frequently asked of forensic practitioners is ‘how much force was necessary to inflict this particular wound’, and as with other aspects of knife wound interpretation, this question is not straightforward to answer.
A rough scale of ‘mild pressure’, ‘moderate force’ or ‘extreme force’ is often used, and the pathologist or forensic physician may utilise the presence of hilt-guard bruising, or the penetration of bone as a guide to their description of force.
The traditional teaching in forensic medicine, based on research by Knight (1975) and others, suggested that the only resistance offered by a body to a stabbing implement was that offered by the skin.
Once the skin surface had been breached, the knife would pass through the body with relative ease. It was therefore the sharpness of the knife tip that superseded all other factors (such as momentum and impact velocity) affecting the depth and extent of a stab injury.
Standards for the evaluation of the sharpness of a knife or similar instruments have been published (BS EN ISO 8442-5), and researchers (eg. Andersen et al 1999) have evaluated the puncture resistance of a variety of possible skin simulants, finding that pig skin is stronger than chamois leather under tensile load, but the puncture resistance for the two is almost identical.
These assertions were based on experiments on cadavers using spring-based instrumented knives measuring the amount of force required to pierce skin and various body parts.
The skin covering the chest wall, for example was easier to pierce than that of the abdomen, because of the tightness of the skin stretched over the chest wall like the ‘skin’ of a drum.
Knight found that as little as 5N of force was required to penetrate skin with a sharp knife, and Chadwick et al (1999) found that volunteers could generate up to 2000N of force along the long axis of a blade at impact (more in overhand stabs than thrusts).
The overhand style of stabbing generated more ‘cutting power’, as the knife was dragged down through the skin, and the ‘swipe/ slash’ style generated the largest lateral forces during simulated stabbing attacks.
A common defence assertion is that the victim ‘fell’ onto the knife or that it was an ‘accident’, and Knight’s research seemed to add weight to the validity of some of these claims.
The resistance offered by soft tissues/ muscle fascia etc is now thought to be more significant. Indeed, tissues other than skin can offer resistance enough to slow a moving knife down, requiring the assailant to continue to exert pressure in order to complete a thrust (Horsfall et al 1999; Chadwick et al 1999; O’Callaghan et al 1999).
O’Callaghan et al (1999) found that skin did indeed provide the greatest resistance to penetration (with a mean penetration force of 49.5 N), whilst significant secondary resistive forces were provided by subcutaneous muscle (but not adipose tissue).
They argued that the original research of Knight and Green was not quite accurate, as the spring based instrumented knives used would ‘store’ energy at the point of penetration, which would then be released after penetration, providing a significant amount of energy that would be more than enough to overcome the resistive forces of muscle and fatty tissue, thus giving the impression that the knife was able to pass through such tissues with no appreciable resistance.
The identification of such secondary resistive forces is an important consideration for defences involving thrown knives – the energy possessed by the knife is likely to be dissipated having overcome the resistive forces of skin (and clothing), such that deeper penetration through muscle is less likely.
The subject of the biomechanics in relation to stab injuries is of vital importance to those seeking to protect persons against such injuries, eg. Police services and manufactures of stab-proof clothing. Current research indicates a far more complicated situation than was perhaps previously appreciated.
Cheap kitchen knives can easily break with minimal force, and when such a knife tip strikes bone, the tip may break off, and remain embedded in the bone. X rays of knife wounds and surrounding body parts are thus useful in finding such foreign bodies.
If knife tips are recovered at surgery or during autopsy, they should be retained as trace evidence, and submitted to ‘tool mark’ specialists who may be able to match the fragment to a recovered suspect weapon.
Biomechanical factors that can be assessed in sharp force injuries:
- The properties of the knife
- Movement of the knife up to the point of impact (affected by clothing and movement of the victim (with respect to the assailant), and from the skin to it's termination within the body)
- The speed and direction of delivery of the blow
- Intrinsic properties of the knife - shape/ sharpness/ weight
- Delivery of the blow - velocity/ type of thrust and 'follow through' ('over arm' vs. 'under arm')
- Movement of the knife within the body - affected by skin/ organ resistance, movement of the victim and whether bone has been impacted
activity following stabbing
Post injury survival time estimations are useful in that they can assist in the reconstructive process, and in giving court testimony. However, they cannot be accurately predicted, and several studies have found that stab wound victims are capable of quite strenuous activity post injury infliction.
Levy and Rao (1988) found that 71% of victims survived for more than 5 minutes, and that post injury activity and survival time was not influenced by the degree of alcohol or drug intoxication.
They found that slit-like wounds produced during stabbings led to less massive blood loss, as the wound margins were in close proximity and the elasticity of the tissues helped to tamponade the blood flow.
Unless the stab wound involves the brainstem, death is not instantaneous, and victims of stabbing are capable of energetic actions, such as running and climbing stairs before they collapse.
If the heart or great vessels are targeted, the assault may be enough to ‘drop’ the victim straight away, but consciousness will not necessarily be lost immediately.
Thoresen and Rognum (1986) found that 72% of those who had acting capability following the assault were dead within 30 minutes, and those who sustained penetrating injury to the heart were unlikely to survive longer than 12 hours.
Most victims with heart and great vessel injuries were dead within 1 hour. Purdue (2000) refers to studies that had shown 68% of victims stabbed in the heart surviving (compared to 14% being shot in the heart).
Survival from stab and other incised wounds may therefore rely on prompt trauma care and resuscitation techniques.
references
- Andersen J, Birkbeck AE, Thomson RD, Vanezis P (1999), 'Puncture resistance and tensile strength of skin simulants', Proc Inst Mech Eng [H] 213(6):493-501
- Byard RW, Gehl A, Tsokos M (2005), 'Skin tension and cleavage lines (Langer's lines) causing distortion of ante- and post mortem wound morphology', Int J Legal Med 119:226-230
- Chadwick E.K.J., Nicol A.C., Lane J.V., Gray T.G.F. (1999), ‘Biomechanics of knife stab attacks’, Forensic Science International Vol 105: 35-44
- Ciallella C., Caringi C., Aromatario M. (2002), ‘Wounds inflicted by survival-knives’, Forensic Science International 126(1) 82-87
- Green M.A. (1978), ‘Stab wound dynamics – a recording technique for use in medico-legal investigations’, Journal of Forensic Science Society, Vol 18: 161-163
- Haut RC (1989), 'The effects of orientation and location on the strength of dorsal rat skin in high and low speed tensile failure experiments', Journal of biomechanical engineering', 111 (2):136-146
- Horsfall I., Prosser P.D., Watson C.H., Champion S.M. (1999), ‘An assessment of human performance in stabbing’, Forensic Science International Vol. 102: 79-89
- Hunt A.C., Cowling R.J. (1991), ‘Murder by stabbing’, Forensic Science International, Vol 52:107-112
- Hunt A.C. (2003), ‘Morphology of knife wounds’, Presentation to the British Association in Forensic Medicine Winter Meeting, Cardiff, Wales 29th November 2003
- Karlsson T (1998), ‘Homicidal and suicidal sharp force fatalities in Stockholm, Sweden. Orientation of entrance wounds in stabs gives information in the classification’, Forensic Science International 93(1) 21-32
- Knight B. (1975), ‘The dynamics of stab wounds’, Forensic Science Vol 6: 249-255
- Knight B. (1996), ‘Forensic Pathology’, 2nd Ed, Arnold
- Levy V. and Rao V.J (1988), ‘Survival time in gunshot and stab wound victims’, American Journal of Forensic Medicine and Pathology, Vol 9(3): 215-217
- O’Callaghan P.T., Jones M.D., James D.S., Leadbeatter S., Holt C.A., Noakes L.D.M. (1999), ‘Dynamics of stab wounds: force required for penetration of various cadaveric human tissues’, Forensic Science International 104(2-3): 173-178
- Ormstad K., Karlsson T., Enkler L., Law B., Rajs J. (1986), ‘Patterns in sharp force fatalities – a comprehensive forensic medical study’, Journal of Forensic Sciences Vol 31(2) pp.529-542
- Purdue B.N. (2000), ‘Cutting and piercing wounds’, Chapter 9 in Mason J.K. and Purdue B.N. (Ed), ‘The pathology of trauma’, 3rd Ed, Arnold
- Thali MJ, Schwab CM, Tairi K, Dirnhofer R, Vock P (2002), 'Forensic radiology with cross-section modalities: spiral CT evaluation of a knife wound to the aorta', Journal of Forensic Sciences 47(5):1041-5
- Thoresen S.O. and Rognum T.O. (1986), ‘Survival time and acting capability after fatal injury by sharp weapons’, Forensic Science International, Vol 31: 181-187
complications of stab wounds - retained knives


37-year-old Li Fu, who had complained of severe headaches for 4 years, was recently found to have a 10cm-long knife blade embedded in his head, from a previous assault. Read the story here ...